| Endovenous Laser Treatment (EVLT) |
| |
Significant advances have occurred in the understanding, diagnosis, and management of venous insufficiency over the last decade or so, mostly owing to the use of duplex ultrasound (DUS) technology. DUS is essential prior to treatment in all patients with CEAP C2 or higher venous disease in order to identify reflux and establish the pattern of disease. Venous insufficiency from superficial reflux through varicose veins is a serious problem that usually is inexorably progressive if left untreated. Saphenous vein reflux is the underlying primary abnormality in many patients with superficial venous insufficiency.
The Endovenous Laser Treatment, abbreviated EVLT, is an innovative, minimally invasive laser procedure that provides the best treatment option to those suffering from varicose veins without an extensive recovery period or scarring.
EVLT being used instead of surgery to treat incompetent segments of the GSV, SSV, anterior accessory saphenous vein, and perforators.
Outcomes from EVLT appear to be equal to or better than stripping, with better quality-of-life scores in the postoperative period. EVLT has been shown to correct or significantly improve the hemodynamic abnormality in patients with chronic venous insufficiency (CVI) with superficial venous reflux. Early reports suggest that endovenous ablation techniques, in contrast to surgical stripping, are associated with a low prevalence of neo vascularization. EVLT has been approved by the FDA as a safe alternative to surgical vein stripping procedures. |
| |
|
Technology |
| Endovenous Laser Ablation (EVLA) works by means of thermal destruction of vein wall. Laser energy is delivered to the desired incompetent segment inside the vein through a bare laser fiber that has been passed through a sheath to the desired location. A variety of laser wavelengths are in use for this procedure, including 810, 940, 980, 1064, 1320 and 1450 nm. When the laser is fired, it deposits thermal energy in the blood and vein wall, causing irreversible localized venous tissue damage. The laser is most commonly delivered continuously as the laser fiber is gradually withdrawn along the course of the vein until the entire vessel is treated. |
| |
|
Technique |
Endovenous Laser Therapy (EVLT) is of value in the treatment of incompetent varicose veins (e.g., GSV, SSV, and anterior accessory saphenous veins). Laser introducer catheters can be passed along small and crooked veins, but they cannot be passed along an extremely tortuous vein with ease.
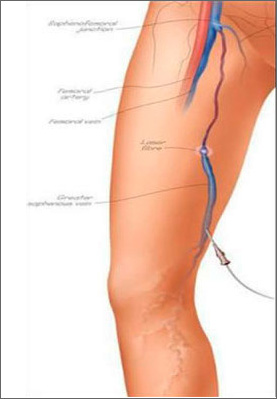
Ultrasonography (USG) is used to confirm and map all areas of reflux and to trace the path of the refluxing great, small, or accessory saphenous trunk from the saphenofemoral or saphenopopliteal junction distally. An appropriate entry point is selected at the distal end of the incompetent segment, at a point that permits cannulation of the vessel with a standard or micropuncture needle introducer. The course of the vein, the junction, and the anticipated entry point are marked on the skin with a surgical marker.
The leg is prepared and draped, and a superficial local anesthetic agent is used to numb the site of cannulation. USG is used to guide the needle puncture of the vessel. The Seldinger technique is used to place a guide wire into the vein, and the guide wire is passed proximally to the sapheno femoral or sapheno popliteal junction. A long introducer sheath (45 cm) is passed over the guide wire, which is then removed.
A 400 µm to 1000 µm sterile, bare-tipped optical fiber is advanced through the sheath until it reaches the end of the sheath. Most laser fibers are marked such that measuring of the fiber is not required. The sheath is then withdrawn over the fiber such that approximately 2-3 cm of bare fiber extends beyond the end of the sheath. With USG guidance, the introducer and laser fibers are slightly withdrawn until the laser tip can be clearly observed approximately 2 cm below the junction. At the saphenofemoral junction, the tip should be just below a competent superficial epigastric vein.
Under USG guidance, a dilute local anesthetic agent is injected into the tissues surrounding the vein to be treated, within its fascial sheath. An anesthetic is injected along the entire course of the vein from the catheter insertion point to the saphenofemoral junction. In most patients, 150-300 mL of lidocaine 0.1% is sufficient to anesthetize and compress the vessel. Delivering the anesthetic in the correct interfascial location with a volume sufficient to compress the vein and dissect it away from other structures along its entire length is important. Some practitioners prefer a local anesthetic with epinephrine, whereas others prefer not to use epinephrine. The procedure is quick and does not cause early postoperative pain, thus long-acting local anesthetic agents are not needed.
USG is used to reconfirm the position of the laser fiber and catheter. Neither the fiber tip nor the laser beam should extend into the femoral vein because injury to the femoral vein may cause deep venous thrombosis (DVT).
When the laser console is switched on, a red aiming beam is visible through the skin. Failure to observe this beam is a reliable indication of malpositioning.
If the vein is small or if the small saphenous vein is being treated, the laser energy may be adjusted to either a lower intensity or a faster pullback.
On rare occasions, the patient experiences momentary pain if the laser is fired in an area with inadequate tumescent anesthesia. Additional delivery of dilute local anesthetic may be indicated.
When the red aiming beam is approximately 2 cm from the entry point, the procedure is complete. The sheath and fiber are withdrawn from the skin, and pressure is applied to the puncture site for a few minutes.
Immediately after the procedure, USG shows a patent vessel that is in spasm through most or all of its length. Follow-up USG at 1 week demonstrates nearly 100% early closure of vessels. |
| |
|
| Tumescent Anesthesia for EVLA |
Transverse ultrasound image of tumescent anesthetic fluid surrounding centrally located great saphenous vein and laser fiber/sheath.
Endovenous Laser Ablation (EVLA) should be performed with the patient under local anesthesia using large volumes of a dilute solution of lidocaine and epinephrine (average volume of 150-300 mL of 0.1% lidocaine without or with 1:1,000,000 epinephrine) that is buffered with sodium bicarbonate. This solution should be delivered either manually or with an infusion pump under ultrasonographic guidance so the vein is surrounded with the anesthetic fluid along the entire length of the segment to be treated. The benefits of tumescent anesthesia for endovenous ablation include the following:
- Anesthesia
- Separation of vein to be treated from surrounding structures
- Thermal sink, which reduces peak temperatures in perivenous tissues
- Vein compression, which maximizes the effect of treatment on the vein wall
Although the maximum safe dosage of lidocaine using a tumescent technique for venous procedures is not well studied, a dosage of 35 mg/kg is a reasonable estimate. Using these parameters, tumescent anesthesia in the context of liposuction has been shown to be extraordinarily safe. |
| |
|
| EVLT Mechanism of Action |
Vein wall injury has been postulated to be mediated both by direct effect and indirectly via laser-induced steam generated by the heating of small amounts of blood within the vein. Some authorities have suggested that the choice of wavelength greatly impacts results.
The main chromophore of 1320-nm lasers (CTEV), at least initially, is water, while other wavelengths used for endovenous laser ablation (EVLA) primarily target hemoglobin. Obviously, adequately damaging the vein wall with thermal energy is imperative in order to obtain effective ablation. Some heating may occur by direct absorption of photon energy (radiation) by the vein wall, as well as by convection from steam bubbles and conduction from heated blood. However, these later mechanisms are unlikely to account for the majority of the impact on the vein.
The maximum temperature of blood is 100°C. Laser treatment has been found to produce carbonization of the vein wall. Carbonization of the laser tip, which occurs at approximately 300°C, is noted following EVLA and seems to occur more frequently with 980nm diode than with 1320 nm Nd:YAG. Carbonization of the laser fiber tip creates a point heat source and essentially reduces light penetration into tissue to zero. |
| |
|
| Follow-Up Care |
Adequate and proper compression is vitally important after any venous procedure. Compression can reduce the (theoretic) risk of venous thromboembolism, and it is also highly effective in reducing postoperative bruising and tenderness. Note that elastic bandages are not an effective means of compression.
Immediately after the procedure, a class II compression stocking (i.e, one with a gradient of 30-40 mm Hg) is applied to the treated leg. Thigh-high– or panty-hose–style stockings are used. The stockings are worn for at least 1 week; they are kept in place continuously for the first 72 hours, but they may be removed for showering thereafter. Bedrest, hot baths, heavy lifting, and long travel are generally forbidden for approximately 1 week, but aerobic activity is encouraged.
Two preliminary reports from 2007 explore the utility of thigh compression after endovenous ablation. The mean pressure of a class II compression stocking is approximately 15 mm Hg at the thigh level, while short-stretch adhesive bandages achieved a pressure of greater than 40 mm Hg, which is the pressure that has been found to significantly reduce the diameter of the GSV in the thigh.
The author has measured the mean sub-bandage (pad, short-stretch bandage, 30– to 40–mm Hg stocking) pressure in the mid thigh immediately following EVLA. The mean pressure in active standing position was 55.8 mm Hg (44-68 mm Hg) (Steven E Zimmet, MD, RVT, FACPH, unpublished data, 2008). This is adequate to compress the thigh portion of the GSV and may explain the apparent reduction in pain and bruising that occurs with increased compression.
Lugli and colleagues conducted a prospective randomized study to investigate the effect of an eccentric thigh compression technique on postoperative pain after endovenous laser ablation (EVLA). They concluded that eccentric compression significantly reduces postoperative pain. Although the concept of increased thigh compression is antithetical to the idea of graduated compression, it may have clinical utility.
The patient is usually reevaluated between postoperative days 3 and 7, at which time DUS should demonstrate the treated vein to be incompressible and without flow, with no evidence of thrombus in the femoral or popliteal veins.
At 4-6 weeks, an examination should reveal clinical improvement of truncal varices, and an USG evaluation should demonstrate a completely closed vessel and no remaining reflux. If any residual open segments or branch veins are noted, sclerotherapy may be performed under USG guidance. |
| |
|
| Complications |
Reports of major complications following endovenous laser ablation (EVLA) are rare. Rates of DVT, pooled from multiple series, are much lower than 1%. One group reported a rate of thrombus extension into the femoral vein of 7.7%. However, in that study, EVLA, was performed with the patient under general or spinal anesthesia. The fact that patients were not able to ambulate immediately postoperatively may have contributed to the high rate of thrombus extension.
One report described an arteriovenous fistula that developed following EVLA of the short saphenous vein. One patient developed septic thrombophlebitis following EVLA combined with open ligation of perforators and stab phlebectomy. This resolved with antibiotic treatment and debridement. |
| |
|
Outcome |
Proof-of-concept studies, using vein occlusion/ablation as the main surrogate outcome measure, exist for these techniques. Endovenous laser ablation (EVLA) has a successful initial closure rate of 95-100%. The outcomes appear durable, with a persistent closure rate of 94-97%.
Significant improvements in physician-measured outcomes such as venous clinical severity scores (VCSS) scores and air-plethysmography (APG) have been reported following endovenous ablation techniques.
A fundamental advance in medicine is the recognition of the importance of patient-reported measures of quality of life. Several studies have documented significant improvement in quality of life after endovenous treatment, and, comparing endovenous laser with stripping, results generally demonstrate equal or better outcomes with better quality of life in the postoperative period.
Endovenous techniques have largely replaced surgical vein stripping in many countries as the first-line treatment for saphenous incompetence. |
| |
|
| Contraindications to EVLT |
- Allergy to local anesthetic
- Hypercoagulable states
- Infection of the leg to be treated
- Lymphedema
- Nonambulatory patient
- Peripheral arterial insufficiency
- Poor general health
- Pregnancy
- Recent or active venous thromboembolism
- Thrombus or synechiae in the vein to be treated
- Tortuous GSV, possibly making placement of the laser fiber difficult
|
| |
|
| Multimedia |
 |
 |
| Varicose vein before treatment with endovenous laser therapy. |
Varicose vein after treatment with endovenous laser. |
 |
| Transverse ultrasound image of tumescent anesthetic fluid surrounding centrally located great saphenous vein and laser fiber/sheath. |
|
| |
|
| |
 Endovenous Laser Therapy is the state-of-the artalternative to surgical stripping in the treatment of varicose veins. This minimally invasive treatment is a procedure performed using ultrasound guidance and local anesthesia. Laser energy is applied to the inside of the refluxing vein, thereby closing it. Endovenous Laser Therapy is the state-of-the artalternative to surgical stripping in the treatment of varicose veins. This minimally invasive treatment is a procedure performed using ultrasound guidance and local anesthesia. Laser energy is applied to the inside of the refluxing vein, thereby closing it.
Once the abnormal vein is closed, the body absorbs it. Once the vein is closed, the blood that was circulating through the vein is simply rerouted to other healthy veins. The varicose veins that were once filled by the faulty vein will then have less pressure in them and, in some cases, will become smaller. |
| |
|
|
|
|
|